Esperanza, patient platform for women with gynaecological cancers.
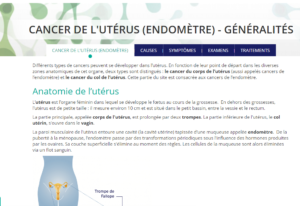
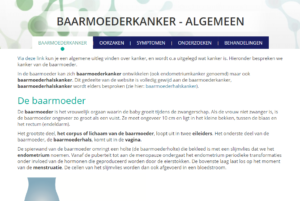
Uterine cancer is a spontaneous malignant growth of cells in the endometrium of the uterus. The endometrium is the mucous membrane lining the uterus, which thickens during the menstrual cycle in preparation for possible implantation of an embryo. Uterine cancer is therefore often referred to as endometrial cancer.
Almost all cases of uterine cancer are endometrial cancer. Only 5% of patients are afflicted by a uterine sarcoma, a rare and aggressive form of uterine cancer where tumours develop in the muscle tissue around the womb.
Uterine cancer concerns the wide, largest part of the actual uterus and is distinguished from cervical cancer, which is restricted to the narrow part of the organ.
Endometrial cancer most often affects women between 50 and 80 years old, only 5% of patients are younger than 50 at the time of diagnosis. In Belgium, around 1500 women are diagnosed with uterine cancer every year, with around 230 women dying from the disease.
Symptoms of patients suffering from uterine cancer partly overlap and coincide with the typical signs associated with menopause. A premenopausal patient may notice irregular and excessive blood loss during periods. For postmenopausal women, vaginal discharge may be a symptom.
Other symptoms associated with uterine or endometrial cancer:
As with most cancers, the exact cause for uterine cancer is unknown, but several factors have been identified that increase the risk of the disease developing:
When a GP suspects a patient may have uterine cancer, they will refer the patient to a gynaecologist who will perform a physical examination and additional tests. This will usually involve a bimanual examination of the vagina and rectum, as well as a speculum examination, in which a cervical smear may be taken. The patient may also be offered a hysteroscopy, which allows the gynaecologist to examine the endometrial lining of the uterus with a micro-camera.
After diagnosis, further tests are needed in order to establish the exact stage the cancer is in. This information will then be used to design the optimum treatment plan for the patient. These tests can include MRI scans, CT scans and thorax X-rays.
To describe uterine cancer, the TNM classification system is used. T stands for the primary tumour, N denotes the occurrence of metastasis in the lymph nodes and M denotes metastasis in other organs of the body.
Four stages
Oncologists define four stages of uterine cancer.
For around three quarters of all women who are diagnosed with cervical cancer, the disease is still in stage I. It is only in the later stages of the disease that the cancer may spread to other organs.
The differentiation of the tumour is an important factor in establishing a prognosis and treatment. This can be determined on the basis of a biopsy. A biopsy involves the removal of a small bit of tissue that can be examined under a microscope. Differentiation determines the degree of mutation in the cancerous cells.
Uterine cancer is usually treated by surgery, radiotherapy, hormone therapy, chemotherapy, or by a combination of these interventions. Surgery generally involves a uterectomy, and in about half of the cases this treatment proves to be efficient. Sometimes internal radiotherapy is also prescribed to prevent a tumour from spreading, whereas patients in more advanced stages of the cancer undergo external radiotherapy. Furthermore, for patients in which it is indicated, targeted therapy with VEGF, mTOR and PD-L1 inhibitors can be used.
Hormone therapy is generally reserved for women who are in stage IV of the illness, as a subsidiary therapy after surgery. Hormone therapy also plays a part in palliative care, when curing the disease is no longer an option and where focus shifts to ensuring the patient’s quality of life. Chemotherapy is often applied during stage I or II of the illness.