Neovida, patient association for people with bladder cancer (Dutch)
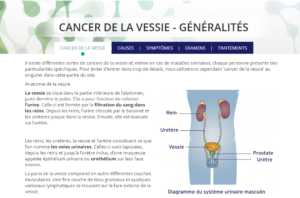
Bladder cancer begins when cells in the urinary bladder start to grow uncontrollably. As more cancer cells develop, they can form a tumour and spread to other areas of the body.
Most bladder cancers (around 90%) start in the innermost lining of the bladder, which is called the urothelium or transitional epithelium. As the cancer grows into or through the other layers in the bladder wall, it becomes more advanced and can be more difficult to treat.
Over time, the cancer might grow outside the bladder and into nearby structures. It might spread to nearby lymph nodes or to other parts of the body. (If bladder cancer spreads, it often goes first to distant lymph nodes, the bones, the lungs or the liver.)
Cancer that develops in the bladder lining is called urothelial cancer or transitional epithelium cancer. Much rarer types of bladder cancer are squamous cell carcinoma or adenocarcinoma.
A growth in the bladder is malignant in 95% of all cases, in the other 5% the grown is known as a polyp.
Two types of bladder cancer are distinguished, based on how far they have invaded into the bladder wall:
In Belgium, around 2500 new cases of bladder cancer are registered every year. Around 80% of all patients are men. In Belgium, bladder cancer is the fifth most prevalent cancer in men. Most patients are over 60 years old.
The five-year survival rate of patients with non-muscle invasive bladder cancer is relatively high around the lower stages of the disease: up to 95% in stage 0 and up to 80% in stage I. For the invasive type of cancer, the outlook is not as good: 51% for a patient in stage II, 12% for stage IV.
One of the first signs of bladder cancer is blood in urine. A greater urge to urinate combined with pain during urination can also be warning signs. Certain symptoms are not directly caused by the tumour, but by the body’s reaction to it. These include fever, fatigue and nightly perspiration.
The cause of bladder cancer is not precisely known, but certain factors have been identified that will raise the risk of contracting the disease.
When a GP suspects a patient may have bladder cancer, they will first have the urine examined and possibly perform a rectal or vaginal examination. When the patient’s blood contains urine, a referral to the urologist follows. The urologist will perform further tests, such as a urine cytology test in which the presence of malignant cells can be established. A cystoscopy examines the inside of the bladder.
When the presence of a tumour has been established, the urologist will perform a transurethral resection of the tumour (TURT) to obtain tumour tissue, after which the cancer type and stage will become apparent. In case of a non-invasive tumour, the patient is assessed as to being low, medium or high risk. Invasive tumours require further tests to establish if the cancer has spread, such as CAT scans, MRI scans or PET scans.
A staging system is a standard way for the cancer care team to describe how far a cancer has spread. The staging system most often used for bladder cancer is the TNM system, which is based on three key pieces of information:
Pinpointing the exact stage of the cancer is also of vital importance when it comes to setting up a treatment plan. There are five stages:
The differentiation of the tumour is an important factor in establishing a prognosis and treatment. This can be determined on the basis of a biopsy. A biopsy involves the removal of a small bit of tissue that can be examined under a microscope. Differentiation determines the degree of mutation in the cancerous cells.
In case of a non-muscle invasive bladder tumour, a TURT treatment can be administered in order to scrape the tumour away. This treatment is usually followed up by one or more lavages. Sometimes these involve cytostatica: medication that kills off cells or stops cell growth. Other lavages can include BCG, a booster to the immune system.
Muscle-invasive tumours are treated in a different manner. When the tumour has metastasised, treatment is limited to palliative care, since healing is no longer an option. If the tumour has not yet advanced to that stage, oncologists have the options of operation, radiotherapy, chemotherapy and immunotherapy. In some cases, several methods are combined in order to enhance the chance of success. In patients with locally advanced or metastatic disease, who express FGFR mutations, targeted therapy with FGFR inhibitors can be used.
When a tumour has reached stage II or higher, a cystectomy (surgical removal of the bladder) is usually performed. In men, this often also involves removal of the prostate, and in women it involves removal of the uterus and/or ovaries. Radiotherapy is often applied when a patient’s condition does not allow for an operation.